Abduction Pillow_applying And Removing 4c516
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 3i3n4
Overview 26281t
& View Abduction Pillow_applying And Removing as PDF for free.
More details 6y5l6z
- Words: 3,147
- Pages: 4
NURSING PRACTICE & SKILL
Abduction Pillow: Applying and Removing What is Applying and Removing an Abduction Pillow? › What: An abduction pillow (also called an abduction splint) is a specially designed wedge-shaped pillow that is used to reduce risk of hip dislocation in patients who have undergone hip arthroplasty (i.e., surgery to replace the hip t with a prosthetic implant). The abduction pillow is placed and secured between the patient’s legs to prevent the patient from moving his/her legs into an adducted position (i.e., moving the legs toward or to the midline) or into a position of internal rotation, which can cause dislocation of the hip prosthesis. The use of an abduction pillow also permits clinicians and other caregivers to turn the patient onto his/her unaffected hip without increasing risk for dislocation of the t prosthesis in the affected hip t. An abduction pillow is used whenever the patient is lying down and is removed for toileting, bathing, and whenever the patient is sitting, standing, ambulating, or attending physical therapy sessions › How: When the patient is in bed, the abduction pillow is placed between the legs and secured with straps to maintain both legs in the abducted position (e.g., moved laterally away from the midline) instead of the adducted position. The straps are loosened and the abduction pillow is removed when the patient is not lying down › Where: Abduction pillows are typically used in inpatient settings and in the home care setting › Who: Because of the need for skilled patient assessment, the abduction pillow is applied and removed by a nurse, physician, or physical therapist. This responsibility cannot be delegated to assistive healthcare staff . Assistive staff can, however, observe the patient for changes in leg-hip alignment or other problems when an abduction pillow is in place, and notify the nurse of these changes so that a nursing intervention can be made if necessary. After receiving postsurgical patient care in an inpatient healthcare setting and education of the patient/family , it is appropriate for the abduction pillow to be applied and removed by family or other caregivers in the home care setting
What is the Desired Outcome of Applying and Removing an Abduction Pillow? › The desired outcome of applying and removing an abduction pillow is to keep patients from adducting their legs after hip arthroplasty to reduce risk of hip dislocation
Why is Applying and Removing an Abduction Pillow Important? › Applying an abduction pillow is important because it reduces risk for dislocation of the femoral head of a newly placed artificial hip prosthesis from the acetabular cup (i.e., socket) of the prosthetic hip t › Prevention of dislocation of the femoral head from the socket of the prosthetic hip t is important because its dislocation can cause pain, interfere with normal function of the prosthetic hip t, and necessitate further surgery to restore function
Author Nathalie Smith, RN, MSN, CNP
Reviewers Darlene A. Strayer, RN, MBA Cinahl Information Systems Glendale, California Nursing Practice Council Glendale Adventist Medical Center Glendale, California
Editor Diane Pravikoff, RN, PhD, FAAN Cinahl Information Systems
September 30, 2011
Facts and Figures › Abductor pillows are widely used in the healthcare setting to promote hip t abduction after surgical repair of a fractured hip. Each year, more than 300,000 persons over age 65 years will fracture a hip in the United States and require hip fracture repair surgery (Centers for Disease Control and Prevention, 2010) › In children following hip surgery, an abduction pillow is sometimes used instead of a hip spica cast (i.e., a fiberglass or plaster cast extending from the torso level to the knees or feet that has an opening in the perineal area to permit patient elimination and the performance of hygiene). Compared with the hip spica cast, the advantages of the abduction pillow include the following (Albrektson et al., 2007): • Increased comfort • Improved access for skin care and toileting • Facilitates neurovascular assessment • Complications such as pressure ulcers and osteopenic disuse fractures are more easily prevented › As an illustration of the advantages described above, the findings of investigators who undertook a retrospective review of the medical records of 32 children who underwent hip surgery during the period 1999–2005 noted that use of an abduction pillow provides appropriate hip t stabilization after hip surgeries. In this study, investigators recorded the method of postoperative immobilization (hip spica cast or the use of an abduction
Published by Cinahl Information Systems, a division of EBSCO Publishing. Copyright©2013, Cinahl Information Systems. All rights reserved. No part of this may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the publisher. Cinahl Information Systems accepts no liability for advice or information given herein or errors/omissions in the text. It is merely intended as a general informational overview of the subject for the healthcare professional. Cinahl Information Systems, 1509 Wilson Terrace, Glendale, CA 91206
pillow with knee immobilizer) and complications for each patient. Of the 32 patients involved in the study, 11 (all of whom had a diagnosis of developmental dysplasia of the hip) were treated using a hip spica cast. In the 21 patients treated with an abduction pillow/knee immobilizer, 4 children (19%) were switched to a hip spica cast due to distal femoral fractures as a result of either vigorous resuscitation during a choking episode, parental preference, to increase immobilization and reduce risk of implant loss of fixation, or to correct unstable hip position after the t repair surgery. Abduction pillows/knee immobilizers provided acceptable treatment in 17 of the children (81%); (Albrektson et al., 2007) • The investigators concluded that one child who was successfully resuscitated after a choking incident might have had a worse outcome if he/she was in a spica cast. When the choking incident occurred, the abduction pillow was easily and quickly removed to allow successful resuscitation, although the child subsequently received a hip spica cast as treatment of a distal femoral fracture that occurred during the resuscitation effort. The investigators concluded that an abduction pillow can provide appropriate hip t stabilization in the majority of cases, but children with osteopenic bone who are at risk for fracture and possible implant failure and those with unstable hip reductions may be best treated with immobilization using a hip spica cast
What You Need to Know Before Applying and Removing an Abduction Pillow › The most common indications for hip t arthroplasty are to relieve pain caused by arthritis, correct deformity of the hip t, and restore range of motion and function after disease or injury of the hip t • To reduce the risk of displacement of the hip prosthesis, patients should avoid ive and active adduction and active abduction for at least the first 6 weeks following surgery. To promote this activity restriction, the abduction pillow is used to provide lower limb abduction whenever patients are lying down › Following hip t arthroplasty, patients are allowed gentle (e.g., 20–30º) internal and external rotation of the affected lower extremity and ive abduction as tolerated. Flexing the hip t to an angle of 80–90º for sitting, fully extending the affected leg, and ambulating with assistance is also appropriate • Abduction pillows are typically used for 6–12 weeks until the t capsule has reformed around the hip t and the musculature around the t is sufficiently strengthened to allow proprioceptive control and t stability • Patients who have had previous hip surgery are at higher risk for dislocation and often require longer-term use of an abduction pillow › An abduction pillow is a wedge-shaped device made of sturdy foam that is designed to conform to the inner aspects of the legs. For proper placement of the abduction pillow, the wider bottom edge should be aligned with the ankles and the top edge should be approximately halfway up the thigh. The abduction pillow should extend no higher than halfway up the patient’s thigh in order to avoid pressure on the genital area • Commercially available abduction pillows include a single pediatric size and small, medium, large, and extra large adult sizes. Velcro or buckle closures allow abduction pillows to be adjusted to fit most patients • The most commonly used type of abduction pillow is secured to both legs by two wide straps that are placed across the upper and lower legs. Other models of abduction pillows contain separate straps for each leg. This Nursing Practice & Skill describes the process of applying the most commonly used type of abduction pillow • Abduction pillows are easy to remove for skin care, bathing, neurovascular assessment, and when the patient is not lying down › Necessary nursing skills and areas of nursing knowledge include the following: • Knowledge of postsurgical patient care • Neurovascular and skin assessment › Preliminary steps that should be performed before applying or removing an abduction pillow include the following: • Review the facility protocol for applying/removing an abduction pillow, if one is available • Review the treating clinician’s order for applying and removing an abduction pillow from a patient’s legs, noting any activity restrictions prescribed for the patient – Note if analgesia is prescribed prior to repositioning activity • Review the manufacturer’s instructions, if available, for the type of abduction pillow to be used • Identify the patient using facility protocol • Ensure completion of facility informed consent documents. The general consent for treatment executed by patients at the outset of ission to a healthcare facility commonly includes provisions for application and removal of an abduction pillow • Review the patient’s medical history and medical record for any allergies (e.g., to latex, medications, or other substances); use alternative materials as appropriate › Gather the following supplies: • Personal protective equipment (PPE; e.g., nonsterile gloves, gown, mask, eye protection). Typically only nonsterile gloves are required for applying or removing an abduction pillow, although other PPE may be necessary if exposure to body fluids is anticipated • Abduction pillow in a size appropriate for the patient (e.g., pediatric size; small, medium, large, or extra large adult size) • A facility-approved pain assessment tool • Prescribed analgesia • Manufacturer’s instructions, if available, for the abduction pillow • Written information, if available, to reinforce verbal education
How to Apply and Remove an Abduction Pillow › Perform hand hygiene › Don PPE to avoid transfer of microorganisms if risk of exposure to body fluids exists › Introduce yourself and assess the coping ability of the patient and family and for knowledge deficits and anxiety regarding applying and removing the abduction pillow • Determine if the patient/family requires special considerations regarding communication (e.g., due to illiteracy, language barriers, or deafness); make arrangements to meet these needs if they are present – Use professional certified medical interpreters, either in person or via phone, when language barriers exist • Explain the procedure, its purpose, and what outcome to expect from the procedure; answer any questions and provide emotional as needed
› ›
›
›
› ›
– Educate the patient/family that the purpose of the abduction pillow is to prevent the patient from moving his/her affected leg toward or past the midline of the body to protect the femoral head of the hip prosthesis from being displaced from the socket of the prosthesis, and that this protective abduction pillow should be in place anytime the patient is lying down. Explain that this activity restriction will continue for at least 6 weeks or for the period of time prescribed by the treating clinician, and that the patient’s in-home caregiver will need to apply and remove the pillow as needed if the patient is discharged to home Assess the patient’s general status, including his/her pain level using a facility-approved pain assessment tool • If appropriate, premedicate patient with prescribed analgesia; allow for therapeutic level to be reached before beginning repositioning of the pillow Provide an explanation of the procedure while applying the abduction pillow, as described below: • Assist the patient into a comfortable supine position with his/her legs extended and abducted from the midline • Place the abduction pillow between the patient’s legs with the narrow end above the knees and the wider end extending to the ankles • Position the pillow so that the two lateral sides of the pillow are in with the inner aspects of the patient’s legs • Fasten the straps of the abduction pillow securely across the upper and lower aspects of both of the patient’s legs according to facility protocol and manufacturer’s instructions – When properly secured, the pillow should be placed snugly enough against the inner aspects of the patient’s legs to cause the pillow to conform to his/her legs and to immobilize his/her knees, with enough space under the straps to allow placement of one finger between the strap and the skin – After the pillow is secured to the patient’s legs, confirm that his/her knees are immobilized by asking him/her to attempt to gently flex his/her knees. If the pillow has been applied appropriately, he/she will be unable to flex his/her knees and will report feeling comfortable with the abduction pillow in place • Place a pillow under the lower legs of the patient to prevent heel pain and skin breakdown in the heel area Provide an explanation of the procedure when removing the abduction pillow, as described below: • Assist the patient into a comfortable supine position • Detach the straps of the abduction pillow • Gently pull the pillow from between the patient’s legs • Store the pillow in a safe, dry location in the patient’s room Observe the following precautions regarding the use of an abduction pillow: • Do not use an abduction pillow that is not an appropriate size for the patient (e.g., too short or too long) • To avoid exerting pressure on the patient’s lower extremity vasculature or peroneal nerve (i.e., a nerve that es along the lateral aspect of each knee), do not fasten the straps too tightly on the abduction pillow • Straps on abduction pillows should be released with caution in patients who are disoriented and/or have a history of hip dislocation After the abduction pillow has been applied or removed, remove PPE, discard appropriately, and perform hand hygiene Document applying or removing the abduction pillow in the patient’s medical record, including • the time the abduction pillow was applied or removed • patient assessment results, including lower extremity neurovascular status and skin assessment every time the patient is turned (every 2 hours or according to facility protocols) • any unexpected events that occurred, whether or not the treating clinician was notified, and interventions performed • patient outcome • all patient/family education
Other Tests, Treatments, or Procedures That May Be Necessary Before or After Applying and Removing an Abduction Pillow › The abduction pillow will be removed during toileting, bathing, physical therapy, and whenever the patient is sitting, standing, or ambulating. The patient will be repositioned at regular intervals while the abduction pillow is in place according to facility protocol and with appropriate staff assistance. Certain precautions regarding repositioning should be followed: • Reposition the patient every 2 hours to prevent pressure on the skin and decrease the risk of developing pressure ulcers • To avoid placing pressure on the operative site and hip prosthesis, do not turn the patient to the operative side. Turning patients with the abduction pillow in place is limited to turning from the supine position to the nonsurgical/unaffected side and back to the supine position. Place pillows behind the patient’s back to maintain his/her position when in a side-lying position • To promote patient safety, do not turn him/her onto the unaffected side unless both legs are strapped securely to the abduction pillow • Assess neurovascular status and the skin integrity of the legs and feet every 4 hours and as needed › Following the inpatient postoperative period, the patient will be discharged from the patient care facility to home or to another healthcare facility (e.g., a rehabilitation facility) for recovery according to orders of the treating clinician
What to Expect After Applying and Removing an Abduction Pillow › The patient will not experience displacement of his/her hip t prosthesis due to active or ive adduction of the affected leg › The presence of the abduction pillow will cause no alterations in neurovascular status to the patient’s lower extremity(s)
Red Flags › The straps of the abduction pillow may be too tight if paleness or cyanosis of the skin of the lower extremities distal to the abduction pillow develops; capillary refill of the lower extremities is delayed (e.g., > 3 seconds for capillary refill); or the patient reports pain, tingling, or numbness in the lower extremities. If these signs and symptoms develop, loosen the straps so you can slip one finger between the straps of the abduction pillow and the patient’s legs. This will allow adequate circulation to the patient’s lower extremities and prevent pressure on the peroneal nerve
What Do I Need to Tell the Patient/Patient’s Family? › Educate the patient/family about what to expect during and after application of the abduction pillow, and what outcome to expect • After demonstrating the application and removal of the abduction pillow to the patient/family/other in-home caregivers, ask whether they understand how to perform the procedure and whether they have any questions. Encourage the family/other in-home caregivers to provide a return demonstration so you can supervise their technique › Educate regarding the following: • How to the treating clinician if questions or problems arise • Signs and symptoms that may indicate the development of complications (e.g., pressure ulcers) after application of the abduction pillow and should be immediately reported to the treating clinician. Signs and symptoms of developing pressure ulcers include paleness, numbness, pain, and/or breakdown of skin over bony prominences in the lower extremity distal to the abduction pillow • Emphasize the importance of keeping scheduled follow-up medical appointments to allow continued medical surveillance of the patient’s condition › Provide written information, if available, to reinforce verbal education
References 1. Albrektson, J., Kay, R. M., Tolo, V. T., & Skaggs, D. L. (2007). Abduction pillow immobilization following hip surgery: A welcome alternative for selected patients. Journal of Children's Orthopaedics, 1(5), 299-305. 2. Burton, M. A., & Ludwig, L. J. M. (2011). Musculoskeletal care. In Fundamentals of nursing care concepts, connections and skills (pp. 596). Philadelphia: F. A. Davis Company. 3. Centers for Disease Control and Prevention. (2010). Hip fractures among older adults. Retrieved September 21, 2011, from http://www.cdc.gov/homeandrecreationalsafety/ falls/adulthipfx.html 4. Dubuisson, W. C. (2010). Orthopedic measures. In A. G. Perry & P. A. Potter (Eds.), Clinical nursing skills & techniques (7th ed., p. 290). St. Louis: Mosby Elsevier. 5. McConnell, E. A. (2001). Applying a hip abduction pillow. Retrieved September 21, 2011, from http://findarticles.com/p/articles/mi_qa3689/is_200112/ai_n9013808/
Abduction Pillow: Applying and Removing What is Applying and Removing an Abduction Pillow? › What: An abduction pillow (also called an abduction splint) is a specially designed wedge-shaped pillow that is used to reduce risk of hip dislocation in patients who have undergone hip arthroplasty (i.e., surgery to replace the hip t with a prosthetic implant). The abduction pillow is placed and secured between the patient’s legs to prevent the patient from moving his/her legs into an adducted position (i.e., moving the legs toward or to the midline) or into a position of internal rotation, which can cause dislocation of the hip prosthesis. The use of an abduction pillow also permits clinicians and other caregivers to turn the patient onto his/her unaffected hip without increasing risk for dislocation of the t prosthesis in the affected hip t. An abduction pillow is used whenever the patient is lying down and is removed for toileting, bathing, and whenever the patient is sitting, standing, ambulating, or attending physical therapy sessions › How: When the patient is in bed, the abduction pillow is placed between the legs and secured with straps to maintain both legs in the abducted position (e.g., moved laterally away from the midline) instead of the adducted position. The straps are loosened and the abduction pillow is removed when the patient is not lying down › Where: Abduction pillows are typically used in inpatient settings and in the home care setting › Who: Because of the need for skilled patient assessment, the abduction pillow is applied and removed by a nurse, physician, or physical therapist. This responsibility cannot be delegated to assistive healthcare staff . Assistive staff can, however, observe the patient for changes in leg-hip alignment or other problems when an abduction pillow is in place, and notify the nurse of these changes so that a nursing intervention can be made if necessary. After receiving postsurgical patient care in an inpatient healthcare setting and education of the patient/family , it is appropriate for the abduction pillow to be applied and removed by family or other caregivers in the home care setting
What is the Desired Outcome of Applying and Removing an Abduction Pillow? › The desired outcome of applying and removing an abduction pillow is to keep patients from adducting their legs after hip arthroplasty to reduce risk of hip dislocation
Why is Applying and Removing an Abduction Pillow Important? › Applying an abduction pillow is important because it reduces risk for dislocation of the femoral head of a newly placed artificial hip prosthesis from the acetabular cup (i.e., socket) of the prosthetic hip t › Prevention of dislocation of the femoral head from the socket of the prosthetic hip t is important because its dislocation can cause pain, interfere with normal function of the prosthetic hip t, and necessitate further surgery to restore function
Author Nathalie Smith, RN, MSN, CNP
Reviewers Darlene A. Strayer, RN, MBA Cinahl Information Systems Glendale, California Nursing Practice Council Glendale Adventist Medical Center Glendale, California
Editor Diane Pravikoff, RN, PhD, FAAN Cinahl Information Systems
September 30, 2011
Facts and Figures › Abductor pillows are widely used in the healthcare setting to promote hip t abduction after surgical repair of a fractured hip. Each year, more than 300,000 persons over age 65 years will fracture a hip in the United States and require hip fracture repair surgery (Centers for Disease Control and Prevention, 2010) › In children following hip surgery, an abduction pillow is sometimes used instead of a hip spica cast (i.e., a fiberglass or plaster cast extending from the torso level to the knees or feet that has an opening in the perineal area to permit patient elimination and the performance of hygiene). Compared with the hip spica cast, the advantages of the abduction pillow include the following (Albrektson et al., 2007): • Increased comfort • Improved access for skin care and toileting • Facilitates neurovascular assessment • Complications such as pressure ulcers and osteopenic disuse fractures are more easily prevented › As an illustration of the advantages described above, the findings of investigators who undertook a retrospective review of the medical records of 32 children who underwent hip surgery during the period 1999–2005 noted that use of an abduction pillow provides appropriate hip t stabilization after hip surgeries. In this study, investigators recorded the method of postoperative immobilization (hip spica cast or the use of an abduction
Published by Cinahl Information Systems, a division of EBSCO Publishing. Copyright©2013, Cinahl Information Systems. All rights reserved. No part of this may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the publisher. Cinahl Information Systems accepts no liability for advice or information given herein or errors/omissions in the text. It is merely intended as a general informational overview of the subject for the healthcare professional. Cinahl Information Systems, 1509 Wilson Terrace, Glendale, CA 91206
pillow with knee immobilizer) and complications for each patient. Of the 32 patients involved in the study, 11 (all of whom had a diagnosis of developmental dysplasia of the hip) were treated using a hip spica cast. In the 21 patients treated with an abduction pillow/knee immobilizer, 4 children (19%) were switched to a hip spica cast due to distal femoral fractures as a result of either vigorous resuscitation during a choking episode, parental preference, to increase immobilization and reduce risk of implant loss of fixation, or to correct unstable hip position after the t repair surgery. Abduction pillows/knee immobilizers provided acceptable treatment in 17 of the children (81%); (Albrektson et al., 2007) • The investigators concluded that one child who was successfully resuscitated after a choking incident might have had a worse outcome if he/she was in a spica cast. When the choking incident occurred, the abduction pillow was easily and quickly removed to allow successful resuscitation, although the child subsequently received a hip spica cast as treatment of a distal femoral fracture that occurred during the resuscitation effort. The investigators concluded that an abduction pillow can provide appropriate hip t stabilization in the majority of cases, but children with osteopenic bone who are at risk for fracture and possible implant failure and those with unstable hip reductions may be best treated with immobilization using a hip spica cast
What You Need to Know Before Applying and Removing an Abduction Pillow › The most common indications for hip t arthroplasty are to relieve pain caused by arthritis, correct deformity of the hip t, and restore range of motion and function after disease or injury of the hip t • To reduce the risk of displacement of the hip prosthesis, patients should avoid ive and active adduction and active abduction for at least the first 6 weeks following surgery. To promote this activity restriction, the abduction pillow is used to provide lower limb abduction whenever patients are lying down › Following hip t arthroplasty, patients are allowed gentle (e.g., 20–30º) internal and external rotation of the affected lower extremity and ive abduction as tolerated. Flexing the hip t to an angle of 80–90º for sitting, fully extending the affected leg, and ambulating with assistance is also appropriate • Abduction pillows are typically used for 6–12 weeks until the t capsule has reformed around the hip t and the musculature around the t is sufficiently strengthened to allow proprioceptive control and t stability • Patients who have had previous hip surgery are at higher risk for dislocation and often require longer-term use of an abduction pillow › An abduction pillow is a wedge-shaped device made of sturdy foam that is designed to conform to the inner aspects of the legs. For proper placement of the abduction pillow, the wider bottom edge should be aligned with the ankles and the top edge should be approximately halfway up the thigh. The abduction pillow should extend no higher than halfway up the patient’s thigh in order to avoid pressure on the genital area • Commercially available abduction pillows include a single pediatric size and small, medium, large, and extra large adult sizes. Velcro or buckle closures allow abduction pillows to be adjusted to fit most patients • The most commonly used type of abduction pillow is secured to both legs by two wide straps that are placed across the upper and lower legs. Other models of abduction pillows contain separate straps for each leg. This Nursing Practice & Skill describes the process of applying the most commonly used type of abduction pillow • Abduction pillows are easy to remove for skin care, bathing, neurovascular assessment, and when the patient is not lying down › Necessary nursing skills and areas of nursing knowledge include the following: • Knowledge of postsurgical patient care • Neurovascular and skin assessment › Preliminary steps that should be performed before applying or removing an abduction pillow include the following: • Review the facility protocol for applying/removing an abduction pillow, if one is available • Review the treating clinician’s order for applying and removing an abduction pillow from a patient’s legs, noting any activity restrictions prescribed for the patient – Note if analgesia is prescribed prior to repositioning activity • Review the manufacturer’s instructions, if available, for the type of abduction pillow to be used • Identify the patient using facility protocol • Ensure completion of facility informed consent documents. The general consent for treatment executed by patients at the outset of ission to a healthcare facility commonly includes provisions for application and removal of an abduction pillow • Review the patient’s medical history and medical record for any allergies (e.g., to latex, medications, or other substances); use alternative materials as appropriate › Gather the following supplies: • Personal protective equipment (PPE; e.g., nonsterile gloves, gown, mask, eye protection). Typically only nonsterile gloves are required for applying or removing an abduction pillow, although other PPE may be necessary if exposure to body fluids is anticipated • Abduction pillow in a size appropriate for the patient (e.g., pediatric size; small, medium, large, or extra large adult size) • A facility-approved pain assessment tool • Prescribed analgesia • Manufacturer’s instructions, if available, for the abduction pillow • Written information, if available, to reinforce verbal education
How to Apply and Remove an Abduction Pillow › Perform hand hygiene › Don PPE to avoid transfer of microorganisms if risk of exposure to body fluids exists › Introduce yourself and assess the coping ability of the patient and family and for knowledge deficits and anxiety regarding applying and removing the abduction pillow • Determine if the patient/family requires special considerations regarding communication (e.g., due to illiteracy, language barriers, or deafness); make arrangements to meet these needs if they are present – Use professional certified medical interpreters, either in person or via phone, when language barriers exist • Explain the procedure, its purpose, and what outcome to expect from the procedure; answer any questions and provide emotional as needed
› ›
›
›
› ›
– Educate the patient/family that the purpose of the abduction pillow is to prevent the patient from moving his/her affected leg toward or past the midline of the body to protect the femoral head of the hip prosthesis from being displaced from the socket of the prosthesis, and that this protective abduction pillow should be in place anytime the patient is lying down. Explain that this activity restriction will continue for at least 6 weeks or for the period of time prescribed by the treating clinician, and that the patient’s in-home caregiver will need to apply and remove the pillow as needed if the patient is discharged to home Assess the patient’s general status, including his/her pain level using a facility-approved pain assessment tool • If appropriate, premedicate patient with prescribed analgesia; allow for therapeutic level to be reached before beginning repositioning of the pillow Provide an explanation of the procedure while applying the abduction pillow, as described below: • Assist the patient into a comfortable supine position with his/her legs extended and abducted from the midline • Place the abduction pillow between the patient’s legs with the narrow end above the knees and the wider end extending to the ankles • Position the pillow so that the two lateral sides of the pillow are in with the inner aspects of the patient’s legs • Fasten the straps of the abduction pillow securely across the upper and lower aspects of both of the patient’s legs according to facility protocol and manufacturer’s instructions – When properly secured, the pillow should be placed snugly enough against the inner aspects of the patient’s legs to cause the pillow to conform to his/her legs and to immobilize his/her knees, with enough space under the straps to allow placement of one finger between the strap and the skin – After the pillow is secured to the patient’s legs, confirm that his/her knees are immobilized by asking him/her to attempt to gently flex his/her knees. If the pillow has been applied appropriately, he/she will be unable to flex his/her knees and will report feeling comfortable with the abduction pillow in place • Place a pillow under the lower legs of the patient to prevent heel pain and skin breakdown in the heel area Provide an explanation of the procedure when removing the abduction pillow, as described below: • Assist the patient into a comfortable supine position • Detach the straps of the abduction pillow • Gently pull the pillow from between the patient’s legs • Store the pillow in a safe, dry location in the patient’s room Observe the following precautions regarding the use of an abduction pillow: • Do not use an abduction pillow that is not an appropriate size for the patient (e.g., too short or too long) • To avoid exerting pressure on the patient’s lower extremity vasculature or peroneal nerve (i.e., a nerve that es along the lateral aspect of each knee), do not fasten the straps too tightly on the abduction pillow • Straps on abduction pillows should be released with caution in patients who are disoriented and/or have a history of hip dislocation After the abduction pillow has been applied or removed, remove PPE, discard appropriately, and perform hand hygiene Document applying or removing the abduction pillow in the patient’s medical record, including • the time the abduction pillow was applied or removed • patient assessment results, including lower extremity neurovascular status and skin assessment every time the patient is turned (every 2 hours or according to facility protocols) • any unexpected events that occurred, whether or not the treating clinician was notified, and interventions performed • patient outcome • all patient/family education
Other Tests, Treatments, or Procedures That May Be Necessary Before or After Applying and Removing an Abduction Pillow › The abduction pillow will be removed during toileting, bathing, physical therapy, and whenever the patient is sitting, standing, or ambulating. The patient will be repositioned at regular intervals while the abduction pillow is in place according to facility protocol and with appropriate staff assistance. Certain precautions regarding repositioning should be followed: • Reposition the patient every 2 hours to prevent pressure on the skin and decrease the risk of developing pressure ulcers • To avoid placing pressure on the operative site and hip prosthesis, do not turn the patient to the operative side. Turning patients with the abduction pillow in place is limited to turning from the supine position to the nonsurgical/unaffected side and back to the supine position. Place pillows behind the patient’s back to maintain his/her position when in a side-lying position • To promote patient safety, do not turn him/her onto the unaffected side unless both legs are strapped securely to the abduction pillow • Assess neurovascular status and the skin integrity of the legs and feet every 4 hours and as needed › Following the inpatient postoperative period, the patient will be discharged from the patient care facility to home or to another healthcare facility (e.g., a rehabilitation facility) for recovery according to orders of the treating clinician
What to Expect After Applying and Removing an Abduction Pillow › The patient will not experience displacement of his/her hip t prosthesis due to active or ive adduction of the affected leg › The presence of the abduction pillow will cause no alterations in neurovascular status to the patient’s lower extremity(s)
Red Flags › The straps of the abduction pillow may be too tight if paleness or cyanosis of the skin of the lower extremities distal to the abduction pillow develops; capillary refill of the lower extremities is delayed (e.g., > 3 seconds for capillary refill); or the patient reports pain, tingling, or numbness in the lower extremities. If these signs and symptoms develop, loosen the straps so you can slip one finger between the straps of the abduction pillow and the patient’s legs. This will allow adequate circulation to the patient’s lower extremities and prevent pressure on the peroneal nerve
What Do I Need to Tell the Patient/Patient’s Family? › Educate the patient/family about what to expect during and after application of the abduction pillow, and what outcome to expect • After demonstrating the application and removal of the abduction pillow to the patient/family/other in-home caregivers, ask whether they understand how to perform the procedure and whether they have any questions. Encourage the family/other in-home caregivers to provide a return demonstration so you can supervise their technique › Educate regarding the following: • How to the treating clinician if questions or problems arise • Signs and symptoms that may indicate the development of complications (e.g., pressure ulcers) after application of the abduction pillow and should be immediately reported to the treating clinician. Signs and symptoms of developing pressure ulcers include paleness, numbness, pain, and/or breakdown of skin over bony prominences in the lower extremity distal to the abduction pillow • Emphasize the importance of keeping scheduled follow-up medical appointments to allow continued medical surveillance of the patient’s condition › Provide written information, if available, to reinforce verbal education
References 1. Albrektson, J., Kay, R. M., Tolo, V. T., & Skaggs, D. L. (2007). Abduction pillow immobilization following hip surgery: A welcome alternative for selected patients. Journal of Children's Orthopaedics, 1(5), 299-305. 2. Burton, M. A., & Ludwig, L. J. M. (2011). Musculoskeletal care. In Fundamentals of nursing care concepts, connections and skills (pp. 596). Philadelphia: F. A. Davis Company. 3. Centers for Disease Control and Prevention. (2010). Hip fractures among older adults. Retrieved September 21, 2011, from http://www.cdc.gov/homeandrecreationalsafety/ falls/adulthipfx.html 4. Dubuisson, W. C. (2010). Orthopedic measures. In A. G. Perry & P. A. Potter (Eds.), Clinical nursing skills & techniques (7th ed., p. 290). St. Louis: Mosby Elsevier. 5. McConnell, E. A. (2001). Applying a hip abduction pillow. Retrieved September 21, 2011, from http://findarticles.com/p/articles/mi_qa3689/is_200112/ai_n9013808/
Related Documents 3h463d

Abduction Pillow_applying And Removing 4c516
December 2019 40
Donning And Removing Sterile Gloves 2z6j60
October 2019 34
Kidnapping And Abduction In Ipc 5b4u2f
December 2019 69
Cold Case Abduction 446z3f
September 2021 0
Fw Removing White Backgrounds 345m39
December 2019 35
Gfi Agent Removing Procedure 2b172z
November 2019 37More Documents from "Pedro Gaspar" 2n1d3k
Abduction Pillow_applying And Removing 4c516
December 2019 40
308 75 Viajante De Comercio1 443h57
June 2022 0
A Arte Da Nao Conformidade - Chris Guillebeau 4gt6g
November 2019 116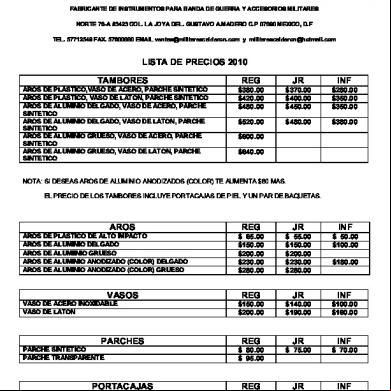
Precios Calderon 4d1e19
December 2019 52
Nexos Causales 494p49
November 2019 71