Physical Therapy Skills Checklist 471h2a
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 3i3n4
Overview 26281t
& View Physical Therapy Skills Checklist as PDF for free.
More details 6y5l6z
- Words: 704
- Pages: 4
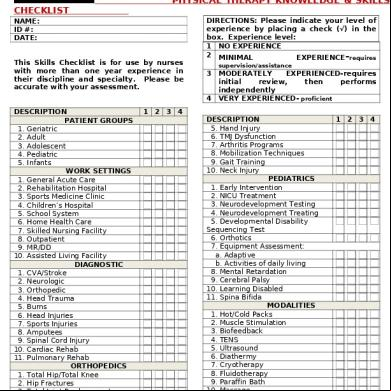
PHYSICAL THERAPY KNOWLEDGE & SKILLS CHECKLIST NAME: ID #: DATE: This Skills Checklist is for use by nurses with more than one year experience in their discipline and specialty. Please be accurate with your assessment.
DIRECTIONS: Please indicate your level of experience by placing a check (√) in the box. Experience level: 1 NO EXPERIENCE 2 MINIMAL EXPERIENCE-requires supervision/assistance
3 4
DESCRIPTION PATIENT GROUPS 1. Geriatric 2. Adult 3. Adolescent 4. Pediatric 5. Infants WORK SETTINGS 1. General Acute Care 2. Rehabilitation Hospital 3. Sports Medicine Clinic 4. Children’s Hospital 5. School System 6. Home Health Care 7. Skilled Nursing Facility 8. Outpatient 9. MR/DD 10. Assisted Living Facility DIAGNOSTIC 1. CVA/Stroke 2. Neurologic 3. Orthopedic 4. Head Trauma 5. Burns 6. Head Injuries 7. Sports Injuries 8. Amputees 9. Spinal Cord Injury 10. Cardiac Rehab 11. Pulmonary Rehab ORTHOPEDICS 1. Total Hip/Total Knee 2. Hip Fractures 3. Total t Replacement 4. Back Syndrome 1 | Page
1 2 3 4
MODERATELY EXPERIENCED-requires initial review, then performs independently VERY EXPERIENCED- proficient
DESCRIPTION 5. Hand Injury 6. TMJ Dysfunction 7. Arthritis Programs 8. Mobilization Techniques 9. Gait Training 10. Neck Injury PEDIATRICS 1. Early Intervention 2. NICU Treatment 3. Neurodevelopment Testing 4. Neurodevelopment Treating 5. Developmental Disability Sequencing Test 6. Orthotics 7. Equipment Assessment: a. Adaptive b. Activities of daily living 8. Mental Retardation 9. Cerebral Palsy 10. Learning Disabled 11. Spina Bifida MODALITIES 1. Hot/Cold Packs 2. Muscle Stimulation 3. Bio 4. TENS 5. Ultrasound 6. Diathermy 7. Cryotherapy 8. Fluidotherapy 9. Paraffin Bath 10. Massage 11. Traction: a. Cervical
1 2 3 4
PHYSICAL THERAPY KNOWLEDGE & SKILLS CHECKLIST NAME: ID #: DATE:
5. 6. 7. 8.
DESCRIPTION 1 2 3 4 MODALITIES (CONT) b. Lumbar 12. Wound Dressing 13. Hydrotherapy a. Hubbard Tank b. Therapeutic Pool c. Whirlpool 14. Myofacial Release Techniques NEUROLOGIC 1. Stroke Rehabilitation 2. Head Trauma 3. Coma Management 4. Spinal Cord Injury PROSTHETICS/ORTHOTICS 1. AK Prosthetics 2. BK Prosthetics 3. UE Prosthetics 4. Orthoplast 5. Resting Splints 6. AFO/PLS 7. Static Splinting 8. Dynamic Splinting 9. Serial/ Inhibitory Casting SPORTS MEDICINE 1. Cybex 2. Biodex 3. Orthotron/Kinetron 4. Lido 5. Nautilus/Eagle 6. Taping/Strapping 7. Strength/ Endurance Training 8. Bracing t Immobilization OTHER 1. Wheelchair: a. Seating b. Ordering 2. Burn Management 3. Cardiac Rehabilitation 4. Chest Physiotherapy DESCRIPTION 1 2 3 4
1. 2. 3. 4. 5. 6.
2 | Page
Inservice Education Work Capacity Evaluation Geriatrics Functional Capacity Evaluation COMPUTERIZED CHARTING Cerner Eclipsys Epic McKesson Meditech Other:
PHYSICAL THERAPY KNOWLEDGE & SKILLS CHECKLIST Name:
MY EXPERIENCE IS PRIMARILY IN:
Please check the boxes below for each age group for which you have expertise in providing age-appropriate nursing care. A. Newborn/Neonatal (birth – 30 days) B. Infant (30 days – 1 year) C. Toddler (1 – 3 years) D. Preschool (3 – 5 years) E. School Age Children (5 – 12 years) F. Adolescent (12 – 18 years) G. Young Adults (18 – 39 years) H. Middle Adults (40 – 64 years) I. Older Adults (64 + years)
B
C
D
E
F
G
H
I
2. Able to adapt care according to normal growth and development. A
B
C
D
E
F
G
years years years years years years
I HAVE CURRENT CERTIFICATIONS FOR:
EXPERIENCE WITH AGE GROUPS: 1. Able to assess age appropriate behavior, motor skills and physiological norms. A
NEUROLOGY PULMONARY SURGICAL MEDICAL CARDIAC CARE TELEMETRY
H
I
3. Able to communicate and instruct patient according to their age, maturity and comprehension ability.
TYPE DATE (MM/DD/YY) ARRHYTHMIA CRITICAL CARE ACLS BLS TNCC NRP PALS NALS Other Other Other Other
COURSE
The information I have provided in this knowledge and skills checklist it true and accurate to the best of my knowledge. Signature
Date
(Written/Electronic)
A
B
C
D
E
F
G
H
I
4. Able to provide a safe environment according to the specific needs of various age groups. A
B
C
D
E
F
G
H
I
ID #: This skills checklist has been reviewed and approved by Nicole Bloxham, RN. Signature
(Written/Electronic)
ID #: Please return to: Company, PA
3 | Page
Date
Northwest
Nurse
Staffing
PHYSICAL THERAPY KNOWLEDGE & SKILLS CHECKLIST ATTN: Records Dept. Fax: (866) 352-4338 Email: [email protected]
4 | Page
DIRECTIONS: Please indicate your level of experience by placing a check (√) in the box. Experience level: 1 NO EXPERIENCE 2 MINIMAL EXPERIENCE-requires supervision/assistance
3 4
DESCRIPTION PATIENT GROUPS 1. Geriatric 2. Adult 3. Adolescent 4. Pediatric 5. Infants WORK SETTINGS 1. General Acute Care 2. Rehabilitation Hospital 3. Sports Medicine Clinic 4. Children’s Hospital 5. School System 6. Home Health Care 7. Skilled Nursing Facility 8. Outpatient 9. MR/DD 10. Assisted Living Facility DIAGNOSTIC 1. CVA/Stroke 2. Neurologic 3. Orthopedic 4. Head Trauma 5. Burns 6. Head Injuries 7. Sports Injuries 8. Amputees 9. Spinal Cord Injury 10. Cardiac Rehab 11. Pulmonary Rehab ORTHOPEDICS 1. Total Hip/Total Knee 2. Hip Fractures 3. Total t Replacement 4. Back Syndrome 1 | Page
1 2 3 4
MODERATELY EXPERIENCED-requires initial review, then performs independently VERY EXPERIENCED- proficient
DESCRIPTION 5. Hand Injury 6. TMJ Dysfunction 7. Arthritis Programs 8. Mobilization Techniques 9. Gait Training 10. Neck Injury PEDIATRICS 1. Early Intervention 2. NICU Treatment 3. Neurodevelopment Testing 4. Neurodevelopment Treating 5. Developmental Disability Sequencing Test 6. Orthotics 7. Equipment Assessment: a. Adaptive b. Activities of daily living 8. Mental Retardation 9. Cerebral Palsy 10. Learning Disabled 11. Spina Bifida MODALITIES 1. Hot/Cold Packs 2. Muscle Stimulation 3. Bio 4. TENS 5. Ultrasound 6. Diathermy 7. Cryotherapy 8. Fluidotherapy 9. Paraffin Bath 10. Massage 11. Traction: a. Cervical
1 2 3 4
PHYSICAL THERAPY KNOWLEDGE & SKILLS CHECKLIST NAME: ID #: DATE:
5. 6. 7. 8.
DESCRIPTION 1 2 3 4 MODALITIES (CONT) b. Lumbar 12. Wound Dressing 13. Hydrotherapy a. Hubbard Tank b. Therapeutic Pool c. Whirlpool 14. Myofacial Release Techniques NEUROLOGIC 1. Stroke Rehabilitation 2. Head Trauma 3. Coma Management 4. Spinal Cord Injury PROSTHETICS/ORTHOTICS 1. AK Prosthetics 2. BK Prosthetics 3. UE Prosthetics 4. Orthoplast 5. Resting Splints 6. AFO/PLS 7. Static Splinting 8. Dynamic Splinting 9. Serial/ Inhibitory Casting SPORTS MEDICINE 1. Cybex 2. Biodex 3. Orthotron/Kinetron 4. Lido 5. Nautilus/Eagle 6. Taping/Strapping 7. Strength/ Endurance Training 8. Bracing t Immobilization OTHER 1. Wheelchair: a. Seating b. Ordering 2. Burn Management 3. Cardiac Rehabilitation 4. Chest Physiotherapy DESCRIPTION 1 2 3 4
1. 2. 3. 4. 5. 6.
2 | Page
Inservice Education Work Capacity Evaluation Geriatrics Functional Capacity Evaluation COMPUTERIZED CHARTING Cerner Eclipsys Epic McKesson Meditech Other:
PHYSICAL THERAPY KNOWLEDGE & SKILLS CHECKLIST Name:
MY EXPERIENCE IS PRIMARILY IN:
Please check the boxes below for each age group for which you have expertise in providing age-appropriate nursing care. A. Newborn/Neonatal (birth – 30 days) B. Infant (30 days – 1 year) C. Toddler (1 – 3 years) D. Preschool (3 – 5 years) E. School Age Children (5 – 12 years) F. Adolescent (12 – 18 years) G. Young Adults (18 – 39 years) H. Middle Adults (40 – 64 years) I. Older Adults (64 + years)
B
C
D
E
F
G
H
I
2. Able to adapt care according to normal growth and development. A
B
C
D
E
F
G
years years years years years years
I HAVE CURRENT CERTIFICATIONS FOR:
EXPERIENCE WITH AGE GROUPS: 1. Able to assess age appropriate behavior, motor skills and physiological norms. A
NEUROLOGY PULMONARY SURGICAL MEDICAL CARDIAC CARE TELEMETRY
H
I
3. Able to communicate and instruct patient according to their age, maturity and comprehension ability.
TYPE DATE (MM/DD/YY) ARRHYTHMIA CRITICAL CARE ACLS BLS TNCC NRP PALS NALS Other Other Other Other
COURSE
The information I have provided in this knowledge and skills checklist it true and accurate to the best of my knowledge. Signature
Date
(Written/Electronic)
A
B
C
D
E
F
G
H
I
4. Able to provide a safe environment according to the specific needs of various age groups. A
B
C
D
E
F
G
H
I
ID #: This skills checklist has been reviewed and approved by Nicole Bloxham, RN. Signature
(Written/Electronic)
ID #: Please return to: Company, PA
3 | Page
Date
Northwest
Nurse
Staffing
PHYSICAL THERAPY KNOWLEDGE & SKILLS CHECKLIST ATTN: Records Dept. Fax: (866) 352-4338 Email: [email protected]
4 | Page
Related Documents 3h463d
Physical Therapy Skills Checklist 471h2a
December 2019 109
Iv Therapy Skills Checklist 2qq6s
December 2019 40
Documentation In Physical Therapy 4l2x12
November 2019 66
Approved Physical Therapy Abbreviations 5t3ts
November 2019 28
Physical Therapy Initial Evaluation 26144k
November 2019 79