Pre Medical Examination Format ( Mer Form ) 4i26u
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report 3i3n4
Overview 26281t
& View Pre Medical Examination Format ( Mer Form ) as PDF for free.
More details 6y5l6z
- Words: 596
- Pages: 5
Star Health and Allied Insurance Co. Ltd. MEDICAL EXAMINATION REPORT (To be filled in by the Medical Examiner) Name of the person to be insured: ____________________________________________________________________ Date of birth: _________________
Age: _____________
Sex:
Marital Status: ________________ Occupation: _____________________________________ Identification Marks:(1) ________________________________________(2)_________________________________ 1. Measurement & Vitals Height(Cms)
BP *
Weight (Kgs)
Systolic
Diastolic
BMI
Waist Circumference (cms)
Pulse Rate /Rhythm
Respiratory rate
I Reading: II Reading: III Reading: *If the Systolic reading is 140 or more or Diastolic reading is 90 or more, second and third reading should be taken with 10 minutes interval of rest. 2. Personal Physician / Last Consultation: Name and address of your personal physician (if none, state the name of the doctor last consulted)
Date of last consultation
Reason
3. Past History Details of medical illness in the past
Period
Details of surgery/procedure undergone in the past
Page 1 of 5
Star Health and Allied Insurance Co. Ltd.
4.(a) If the person to be insured is presently suffering from any of the following diseases, please give details: DISEASE
DURATION & DETAILS OF DRUGS TAKEN
DM/HTN Orthopedics and related diseases
CVA/Neurological Diseases
Heart Disease/Respiratory Illness
Mental Illness
Renal Disease
Cancer
Other (specify)
(b) Within the past 4 years had he/she undergone any diagnostic test like blood test, ECG, CT Scan, MRI etc., If yes, please give details ________________________________________________________________________________
( c ) Details of illness for which OP treatment, IP treatment taken or any check up done during last one year.
Page 2 of 5
Star Health and Allied Insurance Co. Ltd. (d) General Examination Built Nutrition Anaemia Cyanosis Clubbing Pedal edema Lymphadenopathy Others
5. Examination of systems SYSTEMS ENT & Opthalmology Any evidence of cataract or surgery done for cataract (or) Any other visible eye conditions. Are there any missing teeth? If so, give details, Mouth Ulcers, Leucoplakia, etc., Are there DNST/T & A/Ear Discharge & Hearing Loss
YES
NO
DETAILS
Respiratory System. Are there any abnormality or diseases of the respiratory system like TB, Asthma, COPD etc.? Cardiovascular System Is examination of CVS normal ? Abdomen Is there any organomegaly ? Any Ascites Surgical Scar – if any Is there any evidence of Hernia, hydrocele, undescended testis, chronic ulcer etc., Nervous Systems Is there any evidence of neurological disorder such as epilepsy, wasting, involuntary movements, paralysis etc., Muscle Skeletal System Examination of limbs, spine & ts
Page 3 of 5
Star Health and Allied Insurance Co. Ltd. SYSTEMS For female only Is there any disease of the breasts? ( Lump ) Do you suspect any disease of ovaries uterus, cervix
YES
NO
DETAILS
6( a) Family History: Parents If alive Parent Age
Present Health Status
Age at death
If NOT alive Cause of Death
Father
Mother (b) Family History: Diseases of parents If any other family member is suffering from any of the following diseases, please give details Relationship with the person to be insured
DM
HTN
CVA
Heart Disese
Renal Cancer diseases
Mental Illness
Others (Please specify)
Medical Examiner’s Opinion : Are there any Pre-Existing diseases? If yes , give details
Any other remarks.
Page 4 of 5
Star Health and Allied Insurance Co. Ltd.
Is the person to be insured, related or known to Medical Examiner?
Signature of the person to be insured.
Yes/No
Name of the Medical Examiner. Signature & seal.
Place:_________________
Date:____________
Address:____________________________
To be filled in by the Company’s doctor/ doctor Details of pre-existing diseases of the person to be insured to be incorporated in the policy:(1) (2) (3)
Name of doctor: __________________
Signature and Seal: _________________
Place: _______________
Address:____________________________
Date: ____________
________________________________________________________________________________________________
Page 5 of 5
Age: _____________
Sex:
Marital Status: ________________ Occupation: _____________________________________ Identification Marks:(1) ________________________________________(2)_________________________________ 1. Measurement & Vitals Height(Cms)
BP *
Weight (Kgs)
Systolic
Diastolic
BMI
Waist Circumference (cms)
Pulse Rate /Rhythm
Respiratory rate
I Reading: II Reading: III Reading: *If the Systolic reading is 140 or more or Diastolic reading is 90 or more, second and third reading should be taken with 10 minutes interval of rest. 2. Personal Physician / Last Consultation: Name and address of your personal physician (if none, state the name of the doctor last consulted)
Date of last consultation
Reason
3. Past History Details of medical illness in the past
Period
Details of surgery/procedure undergone in the past
Page 1 of 5
Star Health and Allied Insurance Co. Ltd.
4.(a) If the person to be insured is presently suffering from any of the following diseases, please give details: DISEASE
DURATION & DETAILS OF DRUGS TAKEN
DM/HTN Orthopedics and related diseases
CVA/Neurological Diseases
Heart Disease/Respiratory Illness
Mental Illness
Renal Disease
Cancer
Other (specify)
(b) Within the past 4 years had he/she undergone any diagnostic test like blood test, ECG, CT Scan, MRI etc., If yes, please give details ________________________________________________________________________________
( c ) Details of illness for which OP treatment, IP treatment taken or any check up done during last one year.
Page 2 of 5
Star Health and Allied Insurance Co. Ltd. (d) General Examination Built Nutrition Anaemia Cyanosis Clubbing Pedal edema Lymphadenopathy Others
5. Examination of systems SYSTEMS ENT & Opthalmology Any evidence of cataract or surgery done for cataract (or) Any other visible eye conditions. Are there any missing teeth? If so, give details, Mouth Ulcers, Leucoplakia, etc., Are there DNST/T & A/Ear Discharge & Hearing Loss
YES
NO
DETAILS
Respiratory System. Are there any abnormality or diseases of the respiratory system like TB, Asthma, COPD etc.? Cardiovascular System Is examination of CVS normal ? Abdomen Is there any organomegaly ? Any Ascites Surgical Scar – if any Is there any evidence of Hernia, hydrocele, undescended testis, chronic ulcer etc., Nervous Systems Is there any evidence of neurological disorder such as epilepsy, wasting, involuntary movements, paralysis etc., Muscle Skeletal System Examination of limbs, spine & ts
Page 3 of 5
Star Health and Allied Insurance Co. Ltd. SYSTEMS For female only Is there any disease of the breasts? ( Lump ) Do you suspect any disease of ovaries uterus, cervix
YES
NO
DETAILS
6( a) Family History: Parents If alive Parent Age
Present Health Status
Age at death
If NOT alive Cause of Death
Father
Mother (b) Family History: Diseases of parents If any other family member is suffering from any of the following diseases, please give details Relationship with the person to be insured
DM
HTN
CVA
Heart Disese
Renal Cancer diseases
Mental Illness
Others (Please specify)
Medical Examiner’s Opinion : Are there any Pre-Existing diseases? If yes , give details
Any other remarks.
Page 4 of 5
Star Health and Allied Insurance Co. Ltd.
Is the person to be insured, related or known to Medical Examiner?
Signature of the person to be insured.
Yes/No
Name of the Medical Examiner. Signature & seal.
Place:_________________
Date:____________
Address:____________________________
To be filled in by the Company’s doctor/ doctor Details of pre-existing diseases of the person to be insured to be incorporated in the policy:(1) (2) (3)
Name of doctor: __________________
Signature and Seal: _________________
Place: _______________
Address:____________________________
Date: ____________
________________________________________________________________________________________________
Page 5 of 5
Related Documents 3h463d

Pre Medical Examination Format ( Mer Form ) 4i26u
October 2019 323
Qf1-medical-examination-form-medical-certificate.doc 6i2mq
November 2022 0
Gp 69 Form - Medical Examination 6q6x25
October 2019 532
Gp 69 Form Medical Examination 1d6j6h
November 2019 83
Rcl Pre-employment Medical Examination Form B Revised 2015-03 5fj5r
October 2019 175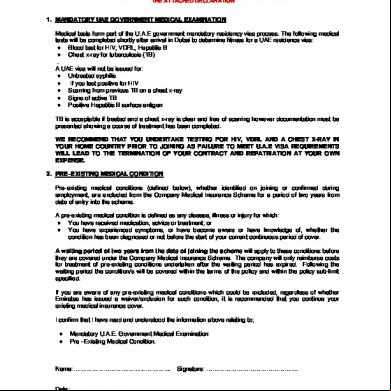
Emirates-pre-employment-medical-examination-form.pdf 6g6n3j
December 2019 45More Documents from "soham" k5s5a
Application Of Chain Drive And Its Selection Method In Automobile 2e4l5x
October 2022 0
Pre Medical Examination Format ( Mer Form ) 4i26u
October 2019 323
November 2019 100

Electronics Note Of Thapar University (first Year) 68y50
December 2019 38
Lathe Drilling Notes 1v3m6y
January 2022 0